Back with an update for you since episode 33 we have Dr Christina Madison, who will give us the latest updates on the Coronavirus.

“BE THE CHANGE”
Gandhi
Listen
[optinform]
Subscribe
iTunes | Stitcher | Google Play | Spotify
What you will learn
- The Latest Update
- How many cases in US and where they are
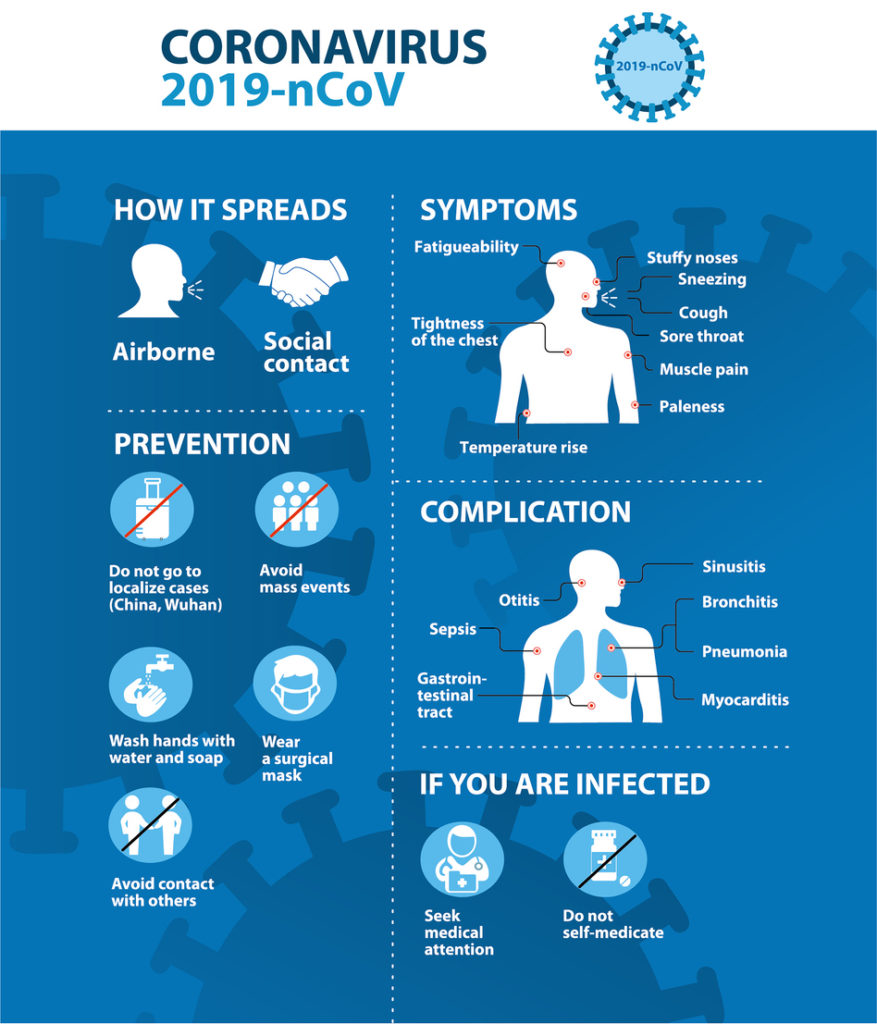
- What are the symptoms
- Know the difference between Influenza and Covid-19
- Pharmacists Guide to Corona Virus
- How do healthcare workers protect themselves
- How do pharmacists & other healthcare workers prevent themselves from getting sick
- The Community Pharmacists Response
Links & Resources
- World Health Organization
- CDC
- EPA List of Disinfectants Active Against COVID-19
- Pharmacists Guide to Corona Virus
- Important steps to Prevent The Corona Virus
- Dr Madison Weighs in on ABC News 13 Las Vegas
- WHO Myth Busters
- WHO Dashboard
- Orange County Healthcare Agency
- Dr Madison’s Publications
- Huntridge Family Clinic Foundation
- Volunteers in Medicine of Southern Nevada
- The Public Health Pharmacist
Subscribe & Review on iTunes
Are you subscribed to our podcast yet? Want to get bonus episodes? Be sure to subscribe so you get notified of any new episode that comes out.
Click here to subscribe on iTunes.
Transcription
Michelle:
This is Michelle Sherman, president of Michelle Rex pharmacist consulting services and your host for the conscious pharmacist podcast, one of the podcasts, part of the pharmacy podcast network. Welcome to today’s episode where we have the public health pharmacist, Dr Christina Madison, back on our show. She was on our show in episode 33 a few weeks ago discussing what’s going on with Kovac 19 the Corona virus. And she’s back on our show today to give us the latest, most current updates of what’s going on with the virus, not only globally, but here in the U S and what you as community pharmacists and pharmacists can do to help your patients. Welcome back to the show. Dr Madison. Thank you so much for having me. Pleasure always. Yes, absolutely. So we’re, we’re weeks into this epidemic now and we’re seeing all this hype on the news on Facebook and Twitter and every way.
Michelle:
And what I’ve witnessed here in Southern California is this mess on slow to grocery stores and places like Costco holding up on water and toilet paper. We can’t get hand sanitizers anywhere. What is going on? Why do we have this kind of mess hysteria going on. And how’s this going to help anything in curtailing the spread of this virus?
Christina:
Yes, that’s an excellent question. I mean at this point we know that our risks in the United States, despite the fact that we have had you know, several cases that have been identified. So there have been 260 cases total for the entire United States, so all 50 States and we’ve seen cases now identified in about 20 States out of the 50 continental United States. I think the reason why people are so panicked is because of the fact that people I have, you know, they, they don’t understand the difference between the symptoms. It feels like it’s this, you know, silent invader that could be creeping or lurking around the corner and, you know, Oh my goodness, you know, I don’t know if I have COVID-19 Oh my gosh, this person coughed next to me. And so unfortunately, because we haven’t seen a really robust public health response as far as messaging to the public about the risk still being low and making sure that, you know, individuals know that even if you have a case that’s been identified in your state or in your County that, you know, just using, you know, good hand hygiene covering your cough, not going to work if you’re sick or ill, you know, wiping down frequently touched surfaces. The EPA actually just released yesterday a list of approved cleaning products that specifically are known to kill COVID-19. So, you know, using those kinds of resources and really listening to reputable, accurate, factual news sources, I think is really the best way for the public to stay informed and making sure that they’re not overreacting.
Christina:
Because ultimately having, you know more toilet paper and more water on hand isn’t going to stop you from getting the virus. What’s gonna stop you from getting the virus is washing your hands and using hand sanitizer and wiping down frequently touched surfaces because you know, you get this from respiratory droplets and the, you know, that the area is about six feet. So, you know, if somebody were to cough or seize on you, if you’re at least six feet away from them, then your risk is, again, it’s low. So I think there’s multiple, you know, streams of information out there that are, you know, slightly inaccurate. The big one would be that people need to wear masks that is not recomended by the CDC for the general public, unfortunately, because we’ve seen people thinking that they need masks. We now have a shortage of them for people who do need them, which are healthcare workers, right?
Christina:
So that what we call PPE or personal protective equipment is in really low supply right now. Luckily the the Trump administration just recently signed an allocations of funding bill yesterday for $8.1 billion specifically for the COVID-19 response. And so I’m hoping that those resources will now be allocated towards getting people and those hospital systems and those primary care clinics, that PPE that they desperately need right now because they’re going to be inundated with people who want to come in and want to be tested.
Michelle:
Exactly. And you know, all this hype and reacting this way when, you know, just simply doing the simple daily, multiple times a day act of washing your hands, just wash your hands go such a long way. And I think in all these public health crises that there’s this one, and I’m sure there’ll be many, many more of the, this is to have some kind of like federal response trickling down from the CDC where all these resources that are so desperately needed by these frontline healthcare workers, the community clinics, the hospitals get the resources right away that they need to be able to take care of the people showing up at their door.
Christina:
Yeah, I mean I’ll just give you my own personal story. I was just at my primary care doctor’s office this morning and they were complaining about the fact that they had no PPE and couldn’t even get a mask. And like they’re the ones who are on the front line, you know they, they, they feel naked. They don’t feel like they’re protected and they don’t feel like they have any, you know, place to turn because everything’s sold out. So, you know, we really do need to ramp up, you know, that protective equipment for, for individuals who are really on the front line, like primary care offices and then also pharmacies, right. Cause people come to the pharmacy sick all the time and there’s really no way for us to know if they have COVID-19 or if they have influenza or if they have a common cold, unless they’re telling us their symptoms.
Christina:
Right. And so I think the big messaging that I’ve been hearing, especially for local and state health departments, is if you really feel like you may have COVID-19, don’t get up and go to the doctor’s office or go to the ER, pick up the phone, pick up the phone, call your doctor, call you know, your, your local health authority go to the CDC website and take that risk assessment and then find out a place where you can go and safely be tested without inundating to health care system. Obviously if you are experiencing severe symptoms such as very high fever and a cough that’s accompanied by marked shortness of breath, then of course we want you to seek medical attention immediately. But for about 80% of people who become infected, they have mild symptoms and those people should not be going to the primary care office.
Christina:
They should be self isolating for that 14 days doing, you know, just general, you know, hydration, cleaning, you know, surfaces keeping themselves as healthy as well and well as they can. And then, you know, just riding the course, obviously if their symptoms become worsened, then they can, you know, seek more advanced medical attention. But that, that’s kind of where we’re at right now. You know, we, we are limited on the number of tests kits that we have. Unfortunately when the CDC originally pushed out the test kits to the local public health labs, they were defective. So the control and the test was not working. And so even if they were using the test appropriately, they couldn’t confirm whether or not it was a true positive because they couldn’t use the control. So we lost about two weeks where we could have been doing more testing because we had to send everything to the CDC. So luckily that that issue has now been corrected, but we’re kind of behind trying to ramp up the, the ability to test now that we’re seeing cases popping up within the United States that are not related to travel or to direct exposure, but really more related to what now we call community spread, which is what we’ve seen in other places of the, of the world, like Italy, Iran in addition to, you know, to China.
Michelle:
And, and you know, you make a great point about people like monitoring their own symptoms and if they’re feeling sick or anything to, to stay home. You know, it’s always amazing to me how people feel like it’s an absolute badge of honor to go to work sick and not only be sick around your coworkers, but the patients that we serve who come in maybe with compromised immune systems and are sick, we can give our patients and our coworkers those illnesses. It’s like no Badge of honor to go out there into the communities, go workout in the gym, go to work and everything. When people feel sick, they should stay home.
Christina:
Yeah, exactly. And, and that’s an interesting point that you bring up because we know that the hourly wage workforce and the service industry that work in like the restaurant industry, that those individuals, it may be more difficult for them to be able to stay home if they’re sick or are some talks right now going on about maybe some stimulus you know, that they could potentially push out for those particular industries where maybe paid sick leave isn’t available. So that they can stay home for that 14 day recommended timeframe. So again depending on what institution you’re at, I’m sure that they have, I’m either COVID-19 response team or task force that they’ve developed. I know here at my university that I work for, we have you know, we have a phase one and a phase two where, you know, planning now based on the fact that we have only had the two identified pieces here in Nevada.
Michelle:
But you know, what do we do if we have to close the school? Like, can we, you know, can we still have classes? Can we still have exams? I mean, these are things that we have to think about. You know, and if you have an older workforce, right? Because we know that those over 50, those with chronic medical conditions are compromised immune systems. Those individuals are more likely to have complications associated with the infection. You may not have the workforce to even support keeping your business open. So, you know, those are the things, those contingency plans, those are the things that businesses need to be thinking about. And, you know, telecommuting and being able to do things from home and really trying to accommodate those workers. Because we’re all going to have to survive this. Right. You know, the, the last thing that I saw was that the projection would be that about 70% of the population will have had COVID-19 within the next year. So even if you haven’t been, quote unquote confirmed, everyone’s gonna have it at some point, right? It’s just who, who are we targeting for more enhanced, you know, protection because they’re higher risks and who, you know, who do we want to, you know, make sure gets those limited resources that we have right now until we can get a vaccine, which is probably still about a year away.
Michelle:
Wow. Yeah, it is. It’s, I mean, this, this is a response where we, we all have responsibility to participate in. What, what can you like from a community pharmacy standpoint, what can we tell a fellow pharmacists out there, especially those working in the community where people are coming up to the counter every single day and having these symptoms and asking what to do. I mean, we as pharmacists are right on the front lines, literally.
Christina:
Absolutely. So the number one thing that I would say is to get with your management and to ask about your ability to use the cleaning services. And I would say that a should be coming in and they should be cleaning down all of the high touch surfaces in the pharmacy at least twice a day minimum. And then having those additional cleaning products inside the pharmacy wiping down computer screens, wiping down keyboards, mouses, your cell phone door knobs for anything that’s frequently touched, have hand sanitizer out and available, not just for yourself, but also for your patients. Don’t shake anyone’s hand. You know, try to keep, you know, if you can that six feet worth of distance, you know, obviously you may have to speak a little louder through the counseling window. But you know, maybe encourage people to use the drive through if possible because at least then you have a bit of a barrier but those kinds of things, you know, cleaning off your pens, you know, cause people use pens all the time.
Christina:
They touch them, right? That’s what the, you know, the virus can live on. It can live on surfaces for up to nine days especially in you know, given the correct, you know, environment. If it’s cold enough and it’s, you know, high humidity, then it can survive for a fairly long period of time. The other thing to to take into consideration is hand-washing. So making sure that you have access to a sink with soap and water. Most pharmacies have a, a bathroom that are inside the pharmacy, cause obviously the pharmacist can’t leave by law. So just frequently washing your hands free, like just continuously and maybe even having a signup that either has that screening criteria from the CDC or having a little comparison chart that says these are the symptoms of COVID-19 versus these are the symptoms of influenza, right?
Christina:
So the big difference is, you know, rapid onset, you know, cough, fever, chills, fatigue, that’s influenza versus COVID-19, anywhere from two to 14 days before you start getting sick. From the time you get exposed, you have a high fever, which is over a hundred and a 100.1 Fahrenheit that’s accompanied by a cough with shortness of breath, right? So knowing the difference between this, the signs of the common cold and the flu versus coven 19, and then having that risk assessment that’s available by the CDC up in your pharmacies so people can, can take their own assessment. And then again, keeping that at least six feet distance if possible. And then wiping down all those services surfaces and making sure that you’re wiping them down with a product that’s been approved for use for COVID-19. And as I mentioned before, the EPA just released that list and I can give you that and you can add that to the show notes for today.
Michelle:
Oh, that’ll be fantastic. Yeah, we’ll definitely edit to all the resources that we listed previously in our previous episode. And we’ll definitely add these today because there’s very, very important information for us as pharmacists to protect ourselves, but you also protect our patients. It’s very important that we spread the message, you know, amongst our colleagues and amongst ourselves that we can better take care of our patients. What do you think about, you know, like travel, like travel? I know people have been saying they’d been going to airport and they like, you’re really quiet. I mean, do you think there’s any risk in flying? None of the, airlines domestically seem to consider that. We see all the international airline warnings like to China and Italy and places like that. But what about the domestically here in the U S.
Christina:
As of right now, there’s no restrictions that have been placed on domestic travel. But again, this is an evolving story. It changes every day. You know, if you had asked me a week ago, I would’ve said there’s no confirmed cases in Nevada. And then yesterday morning I woke up to a text message, you know, from my communications person saying, Hey, we have a presumed positive that’s been identified in Clark County.
Christina:
And then I woke up this morning and heard that there was a second case that had been identified that was associated with the cruise ship that’s now off the coast of San Francisco, that is now living in Washoe County, which is in Northern Nevada. So it’s an evolving story. It’s changing every day. So as of right now, there’s no restriction on domestic travel. Obviously you can go to the CDCs website to check their list of countries that have travel alerts. I know that a lot of the the school systems and the universities because spring break is coming up have now canceled any school sponsored international travel and they’ve been asking anyone who has recently traveled outside of the country to one of those areas that have had higher numbers of COVID-19 cases to self quarantine for the 14 days before coming back to school.
Christina:
So I would say just, you know, check with your local health department you know, check the CDCs website. And you know, the state department has you know, those travel alerts and warnings and advisories up as well. But as of right now, there’s no no restrictions on domestic travel. It’s just those areas where we’ve seen you know, higher amounts of cases. And the one thing to really consider is that even if you don’t want to cancel your travel, that’s fine. Just know that on your way back you may have to self quarantine depending on if the case number changes in that country. So you may be able to go and have your vacation, but coming back you may end up having to self quarantine. So that’s just something to consider as well. And so you know, having trip insurance, making sure that you have access to healthcare there. You know, those should all be considerations for whether or not you decide to take your trip off.
Michelle:
Oh, great. Great information. And I really appreciate you taking time out of your busy schedule. I know you’ve been very busy with all the local TV channels and everything in, in Nevada giving late giving updates like all week long about, about the evolving situation. Before we end off, is there anything else you’d like to add or have the listeners look out for or consider going forward?
Christina:
So the big thing that I would say is, is not to panic. But just to be aware, knowledge is power. And to make sure that you’re going to, you know, reputable sources for your inflammation. And maybe not necessarily taking things from social media because there has been a lot of misinformation that’s been spread about coven 19 and how you can actually get the virus. So just know the facts and make sure that you, you understand what your true risk is. So again, even though as I mentioned before, we’ve had about 260 cases that have been identified in the continental United States. Your risk still remains extremely low. But it’s not a matter of if it’s a matter of when it’s going to come to your state if it’s not there yet. But just know that we have the public health infrastructure in order to handle anything that can happen between now and say the beginning of summer when we’ll probably start seeing a decline in the number of cases because of the warmer weather.
Christina:
You know, we’re working on a vaccine, we’re working on rapid tests that can be done in the ERs and in the primary care clinics. It’s just gonna take time. And the fact that we already have an assay that is readily usable eight weeks from the start of when this virus was identified is pretty incredible when you think about other outbreaks and other diseases that we’ve had in the past. You know, when we think about where we were with H one N one you know, we had no vaccine, no testing for several months. And you know, here we are only eight weeks out and we’re doing extensive testing all over the globe. So I think that’s, that’s where we’re at right now. It’s, you know, we, we have to test people to find it in order to make sure that we stop the spread of the virus. And if you feel like you had symptoms, you know, use that risk assessment tool please don’t panic. Don’t inundate the ERs. You know, let’s, let’s see how this additional funding helps us so that we can get more PPE or personal protective equipment out to the hospital systems and to the primary care clinics so that we can really do our best to handle whatever comes to us and making sure that those who are at at highest risk like the elderly and then, you know, compromise or really getting the care that they need.
Michelle:
Excellent. Well, thank you so much. I really appreciate your time. I know you’re so busy and you know, I know everything my dear. Thank you. I appreciate it. And I know our listeners all the pharmacists and people out there listening on the pharmacy podcast network would, will really appreciate this updated information and again, to all the pharmacists out there we have to be conscious and take this challenge head on because we can make a difference and we can be the change for, for our colleagues pharmacies and, and patients and communities. So thank you Dr Madison for being on the show and we’ll, I hope to see you again soon.
Christina:
Yes, and partner with your local health department. They’re a great resource.
Michelle:
Awesome. Thanks so much.